The catalyst for this lengthy blog post is the recent
news that my province of Ontario is finally, two years later!, seriously considering distinguishing between
causal and
incidental COVID deaths and hospitalizations.
This specific issue has been, for me, the single most significant and neglected issue throughout this whole pandemic. Without transparency on this issue from day 1, the accuracy of the population health threat posed from the virus, which is then utilized to justify the stringent lockdown measures (e.g. school closures) of the past 2+ years, can be questioned. Because most deaths and hospitalizations in general, and those actually caused by this virus, occur in older persons (age >70) it is absolutely essential to make a concerted effort to distinguish between causal and incidental deaths, ICUs and hospitalizations. So I suppose it is better later than never, but this is long overdue.
To show why this is so vital I want to make an analogy with the way in which the province reports "Adverse Events Following Immunization", in particular deaths from the vaccine. I draw attention to this issue not to arm anti-vaxxers with information to perpetuate vaccine hesitancy (the benefits of the vaccine far outweigh the risks, and the adverse events reported are within the normal range for other vaccines), but to show how important it is to distinguish between causal and incidental deaths from both COVID-19 and from vaccines.
Firstly, imagine no serious attempt was made to make a distinction between causal and incidental vaccine deaths. This would mean anyone who happened to die within a few weeks of getting the vaccine, regardless of whether they died in a car crash or of the underlying co-morbidities of advanced age, could be counted as an adverse event. In justifying this odd public health approach health officials remarked "Out of an abundance of caution, we are reporting every conceivable adverse event so that we do not subject people to unsafe medical procedures". If this approach was taken the whole process of immunizations would be undermined, and the population would be left at greater risk of COVID-19 mortality. This approach would be folly because it conflates people who died with the vaccine with those who died from the vaccine. There is a big difference between these two things. And yet this lax approach in reporting deaths and hospitalizations with and from the virus has been taken. I think this was perhaps the biggest mistake of the world's pandemic response, because of the age profile of deaths and serious illnesses (i.e. mostly people over age 70).
OK, so yes we must take great care to distinguish between causal and incidental deaths, whether the issue is death from COVID or from the vaccine. But let us dig deeper. In 2021 the province officially reports that there were 8 fatalities caused by the vaccines, but there are another 26 death cases that are currently listed as "persons under investigation" as they do not clearly meet the province's surveillance definition of death caused by the vaccine. This definition of "death caused by the vaccine" rules out "individuals
with multiple co-morbidities which may be related to the cause of death". Here is the lengthy list of factors that rule out a death from being considered a death caused by the vaccine.
1. Resident of a health-care institution with significant comorbidities. The cause of death was not
attributed to the vaccine.
2. Community dwelling senior with complex cardiovascular and renal conditions, wherein the AEFI
may have contributed to but was not the underlying cause of death.
3. Community dwelling senior with multiple comorbidities including heart disease and an
autoimmune disorder. The cause of death was not attributed to the vaccine.
4. An individual with VITT with death recorded in CCM (described above under Vaccine-Induced
Immune Thrombotic Thrombocytopenia (VITT) and Thrombosis with Thrombocytopenia
Syndrome (TTS) section). A Coroner’s investigation determined that the immediate causes of
death included VITT.
5. Individual with hypertension, wherein the cause of death was not clearly attributed to vaccine.
6. Community dwelling senior with a complex cardiovascular history. The AEFI may have
contributed to but was not the underlying cause of death.
7. Community dwelling senior with multiple comorbidities, wherein the AEFI may have
contributed to but was not the underlying cause of death.
8. Community dwelling senior with severe aortic stenosis. The AEFI may have contributed to but
was not underlying cause of death.
Such scrutiny is certainly justified for without ruling such cases out it would skew our understanding of the safety of the vaccines. However, we should apply a similar diligence to COVID deaths, ICUs and hospitalizations. If we assume everyone who dies with a positive test result for COVID died from COVID, despite the fact that they already had serious underlying health problems, we will get a skewed picture of the pandemic. The same is true for COVID hospitalizations. And this is what has actually happened.
The COVID-19 pandemic has been a novel hybrid pandemic- the virus is both an novel infectious virus AND an emerging disease of aging. I believe the latter has been lost in both the media coverage and the public policy response to this pandemic. And that neglect has meant we responded less effectively than we could have, imposing significant mental health burdens, educational deficits, economic burdens, etc. on younger persons (children and adults age < 50).
I will add one last point to amplify the significance of this insight. At the moment the media headlines are dominated by COVID ICU and hospitalizations numbers. These headlines suggest that it is the unvaccinated that are monopolizing most the hospital beds when it fact it is more accurate to say they are exacerbating the pressures placed on those resources from patients with non-COVID related health problems (the majority of which would be age-related causes- heart attacks, strokes, etc.).
Let us unpack some of the data in Ontario's hospitals, as this goes into greater depth than the typical news story.
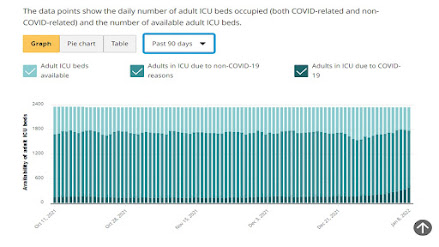
The province has 2343 ICU (adult) beds, of which 1460 beds are for non-COVID patients. I have yet to see a news headline in the past 2 years that discusses the causes, let alone ways to prevent, whatever it is that accounts for 62% of ICU beds for non-COVID patients. At the moment there are 333 people in ICU beds with COVID. This is 14% of the ICU beds, and of those 119 are unvaccinated. So 5% of the ICU beds are being used by unvaccined persons, during the peak of our infection numbers. 550 ICU beds are still available, which means the total ICU bed capacity for adults is at 77% of its full capacity (23% of ICU beds remain available). [as an aside, ICU beds are not fixed and we have had two years to increase capacity vs opting for locking kids and society down as a response to pressures on healthcare resources]. Here is how Canada fares (a bit dated) among other OECD countries:
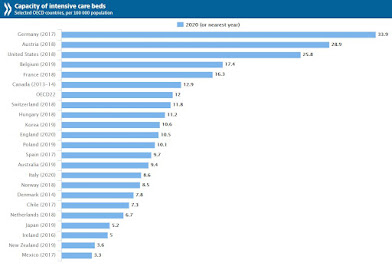
From my perspective, having studied the policy implications of the biology of aging for 15+ years, the popular narrative about the strains caused by the unvaccinated is simply a political distraction from the empirical reality. The reality is that most ICU beds, so far in this pandemic, have been filled mostly with patients that were not hospitalized for COVID. I could not find data on their ages but I would expect most cases are among the older age cohorts (age >60). And of those that do have COVID in (regardless of vaccination status) they are much more likely to be older. This is just one symptom of the much larger health predicament we face with population aging.
This Lancet Public Health piece notes the tsunami of dementia that is coming by the year 2050. Unless we alter our myopic fixation on the proximate causation of disease and death (which this pandemic has further entrenched in the medical sciences and media), we will not be able to meet the health challenges of today's aging world.
Cheers,
Colin